Residential Addiction Treatment Access Equity: Effects of the Medicaid Section 1115 Substance Use Disorder IMD Waiver*
with Helen Newton, Chima Ndumele, David Fiellin, and Susan Busch
For an extension of this work on the underlying mechanism with facility entry and exit dynamics, see my job market paper.
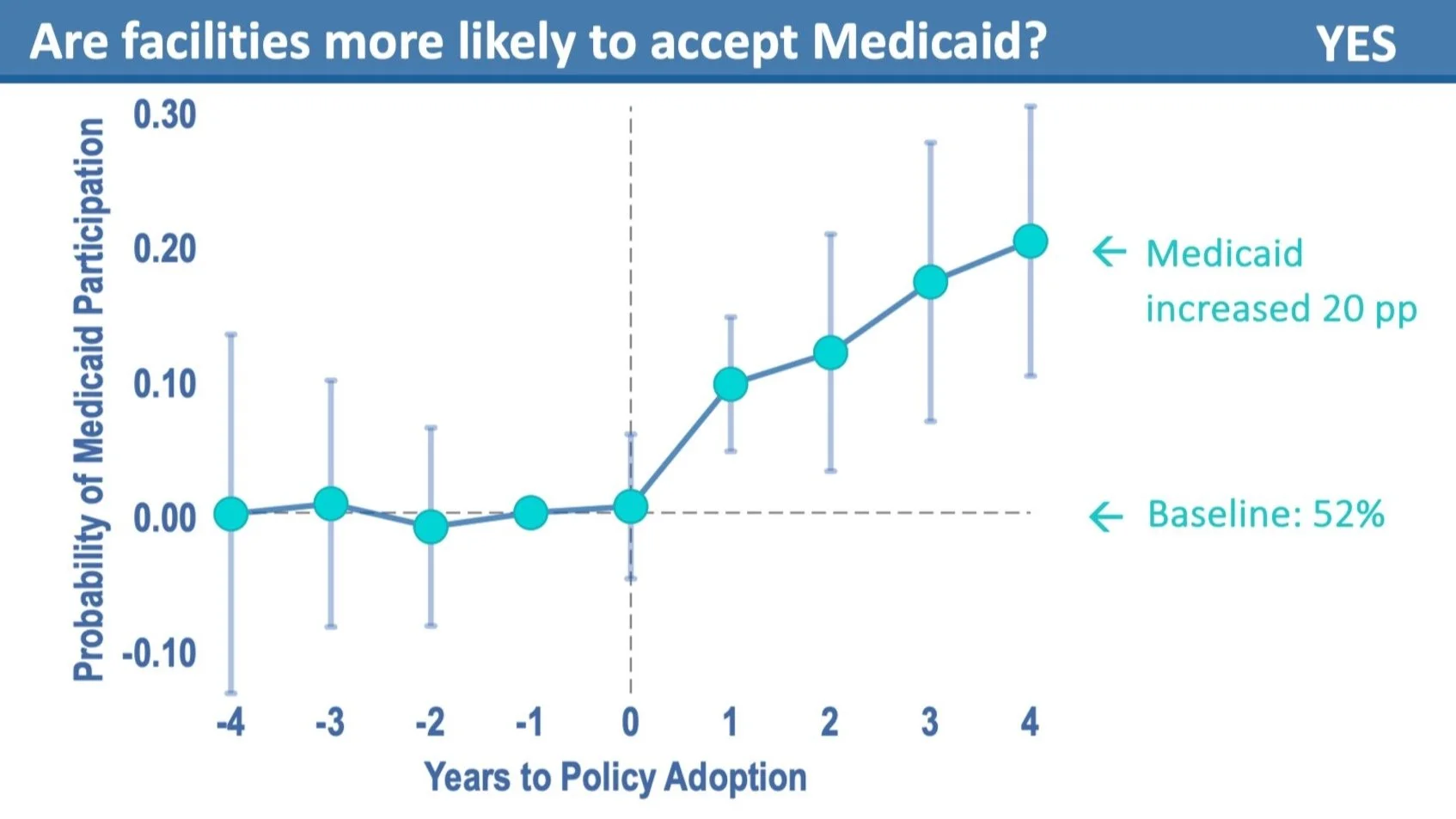
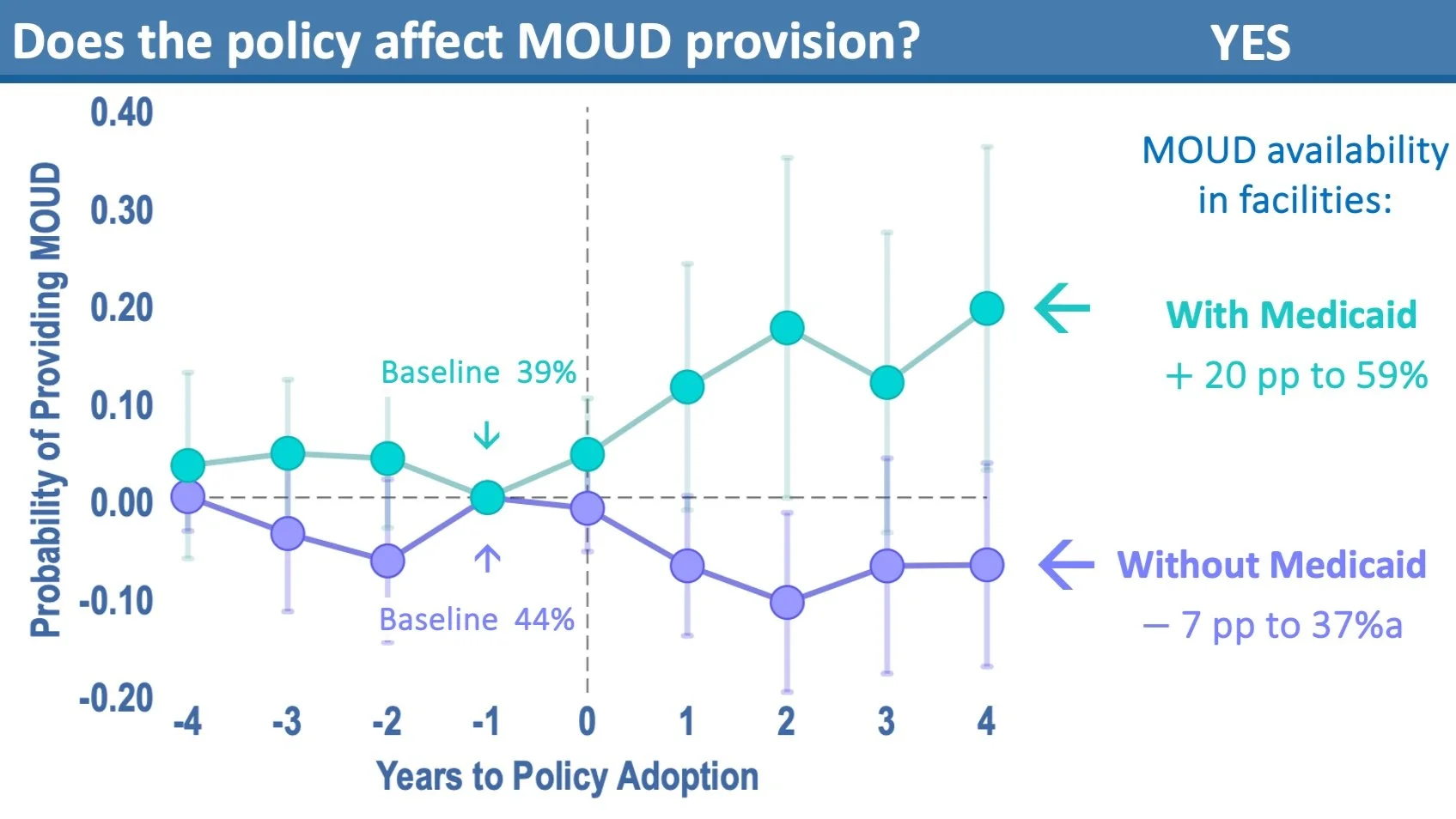
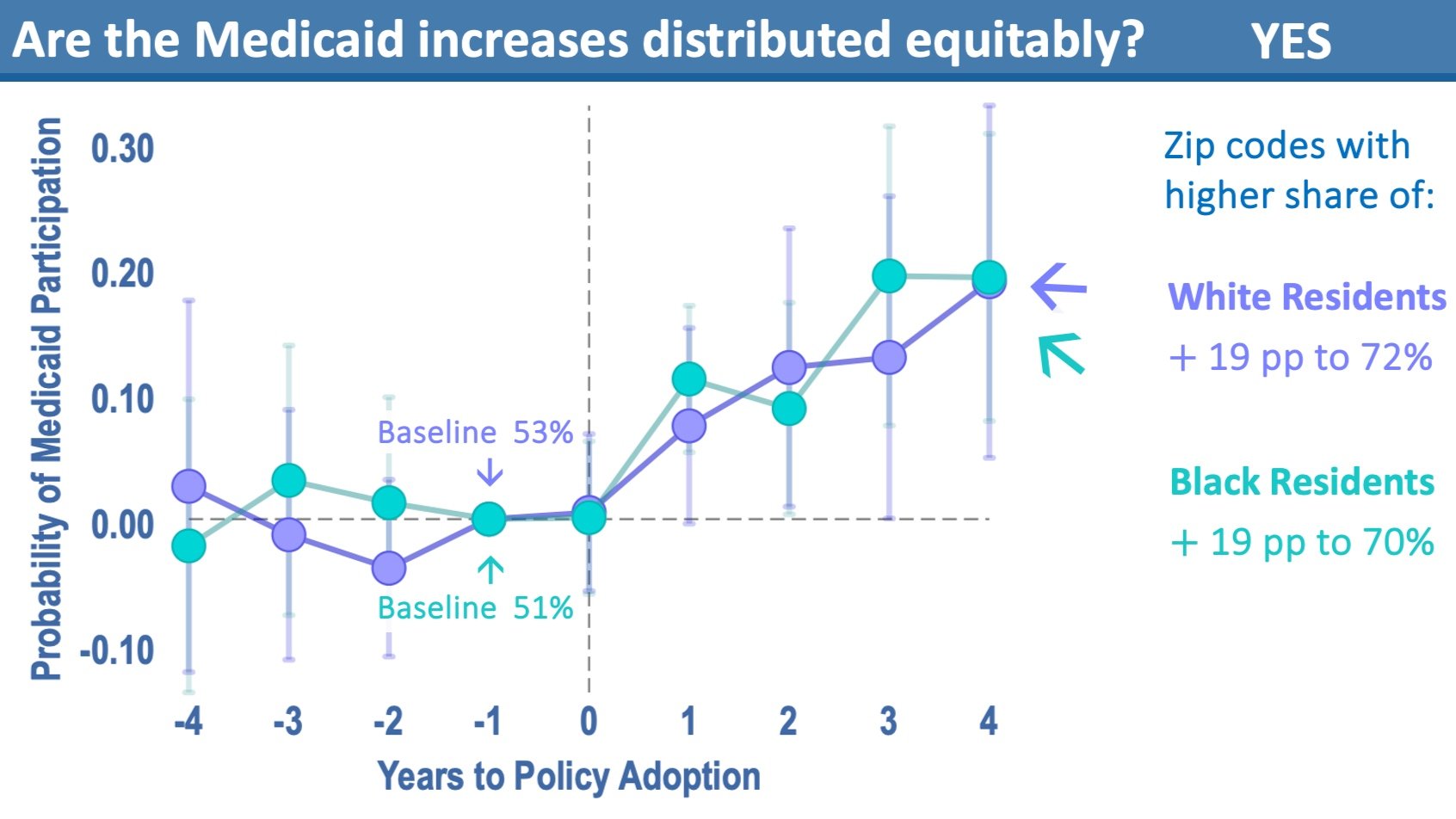
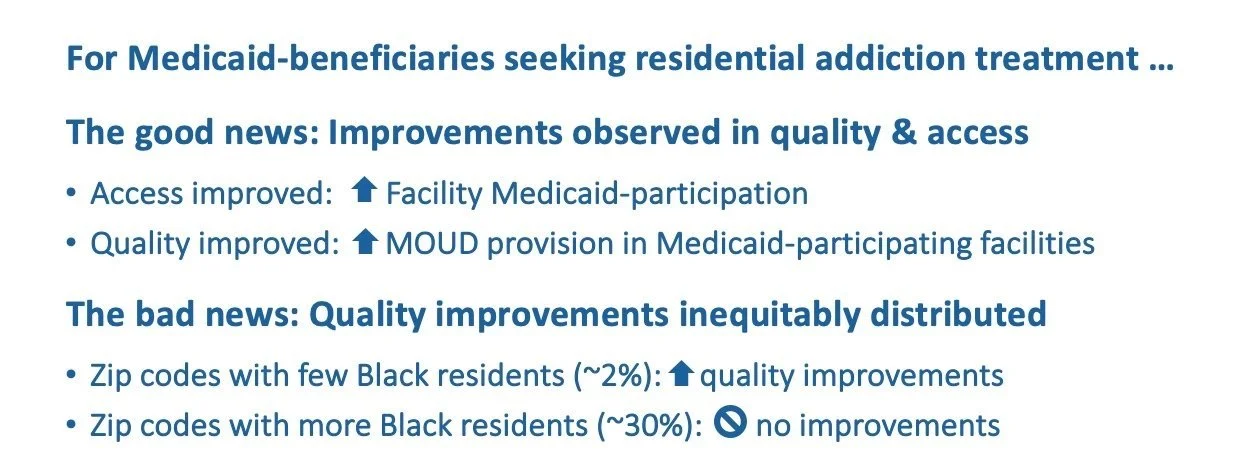
This paper examines the effects of the Medicaid Section 1115 Substance Use Disorder (SUD) IMD Waiver on equitable access to residential addiction treatment in the United States. Medicaid insures a disproportionate share of individuals with opioid use disorder (OUD), including Black individuals who are less likely to receive medications for opioid use disorder (MOUD) despite experiencing the largest increase in opioid-related mortality in recent years. Introduced in 2015, the Section 1115 SUD IMD Waiver allowed states to access federal funding for residential addiction treatment, contingent on meeting new standards intended to improve access and quality of care, including for MOUD, which is underutilized yet can halve the risk of overdose. Using a natural experiment with staggered waiver implementation, we compare outcomes in waiver and non-waiver states from 2009 to 2022. The waiver increased Medicaid acceptance among facilities by 21 percentage points (baseline = 51%) across all communities. However, only facilities in areas with lower shares of Black residents—where Black residents make up about 2% of the population on average—experienced quality improvements, such as increased availability of MOUD. In areas with higher shares of Black residents—where Black residents make up about 30% of the population on average—MOUD availability remained unchanged. These findings highlight the waiver’s potential to improve access to addiction treatment for Medicaid beneficiaries while exposing inequities in the distribution of quality improvements. Section 1115 Waivers are temporary, and Congress is considering permanent national policies to expand addiction treatment. These findings provide the first national evidence on how this policy affects access equity, highlighting the need to address racial disparities in treatment quality as policymakers design future approaches.
*This work received funding from a National Institutes of Drug Abuse Dissertation Award (R36DA058877), National Institutes of Drug Abuse Diversity Supplement (R01DA057789), and the Agency for Healthcare Research and Quality Training Award (T32HS017589).